
|

|
|
 Forensic Neuropathology, 2nd Edition, by Jan E. Leestma. Hard Bound, 10" x 7.2" x 1.3".
Forensic Neuropathology, 2nd Edition, by Jan E. Leestma. Hard Bound, 10" x 7.2" x 1.3".
CRC Press LLC, 2000 Corporate Blvd., N.W., Boca Raton, Florida 33431, Phone - 1(800)272-7737, Fax - 1(800)374-3401. Publication Date October 14, 2008. 768 pages, ISBN-10: 0849391679; ISBN-13: 978-0849391675 (alk. paper). Price: $149.95
 Visit the Official site of this book by clicking here
Visit the Official site of this book by clicking here
Buy from Amazon by clicking here.
 |
 QUICK NOTES QUICK NOTES
Some major highlights of Forensic Neuropathology, 2nd Edition at a glance: |
Leestma's Forensic neuropathology has become a classic over the years. Its first edition came out in 1987, and was immediately accepted as a classic in the field. Now Leestma has come out with a brand new updated edition. Like its predecessor, this new edition comprehensively reviews all aspects of neuropathology that may have forensic or medical-legal importance, but a number of new cases have been added. The book presents significant coverage of the role of the neuropathologist in a legal setting before delving into specific forensic aspects of neuropathology, providing comprehensive discussions of various syndromes and conditions affecting adults and children. It discusses intracranial equilibria and physical injury to the nervous system and contains entire chapters devoted to neuropathology perspectives on child abuse, gunshot and other penetrating wounds of the nervous system, and the forensic aspects of complex neural functions.
The new edition tries to address many common misconceptions in forensic neuropathology. Contributions are included from different disciplines. Kirk Thibault, PhD, a biomechanical engineer with extensive experience in application of physical laws to the study of physical trauma, adds to our understanding of craniocerebral injuries. Proper application of biomechanical principles is crucial to expert witness testimony. Conversely, improper distortion of physical laws needs recognition when such appears in literature or the court. A pathologist is not expected to be a qualified biomechanical engineer but must accept the fact that injurious forces follow laws of physics. The pathologist must be aware of nonmedical contributions made to our understanding of trauma. Ignorant is the pathologist who denigrates the application of biomechanical disciplines to the judging of craniocerebral trauma but accepts erroneous concepts outside the laws of physics.
 |
 |
Chapter 2 entitled "Scientific Evidence and the Courts" has been written by Elaine Whitfield Sharp, JD, an attorney with vast experience on legal issues of injury. The author clarifies for the reader the present legal principles that define expert witness testimony. The legal system in which we operate has developed a framework to judge the worth of expert opinion. However, that method involves the adversary system in which attorneys argue for their side of cause and effect. A forensic pathologist must understand the system and be prepared to present logical and correct justifications of opinions.
Contrasted with some years back, today many physicians tend to include the "intent" aspects of craniocerebral findings in their injury reports. Thus we commonly find terms such as "nonaccidental trauma" or "abusive head trauma" in the injury reports prepapred by emergency physicians. This is perhaps a major impetus for creation of a totally new approach to forensic neuropathology. Dr. Leestma has addressed issues such as these. He approaches this subject in a logical fashion. His comments, supplementd by his co-contributors Dr. Thibault and Ms. Sharp, develop this book into a new and refreshing approach to the interpretation of neuropathology.
I would imagine that this book is a good neuropathology atlas too. I spent lot of time looking at the illustrative pictures, and gained much simply by looking at them. In my opinion, this book should be very useful to forensic pathologists, forensic neuropathologists, clinicians, medical examiners and law enforcement officers.
Leestma has divided his book in nine chapters. The detailed list of contents of this book is as follows:
|
Click here to read an exclusive interview with Dr. Jan Leestma. |
Chapter |
Title |
Author |
Page |
| 1 | Pathology and Neuropathology in the Forensic Setting | Jan E. Leestma, MD, MM and Elaine Whitfield Sharp, JD | 1 |
| 2 | Scientific Evidence and the Courts | Elaine Whitfield Sharp, JD | 27 |
| 3 | Forensic Aspects of Adult General Neuropathology | Jan E. Leestma, MD, MM | 79 |
| 4 | General Forensic Neuropathology of Infants and Children | Jan E. Leestma, MD, MM | 247 |
| 5 | Forensic Aspects of Intracranial Equilibria | Jan E. Leestma, MD, MM | 343 |
| 6 | Physical Injury to the Nervous System | Jan E. Leestma, MD, MM and Kirk L. Thibault, PhD | 399 |
| 7 | Child Abuse: Neuropathology Perspectives | Jan E. Leestma, MD, MM | 561 |
| 8 | Gunshot and Penetrating Wounds of the Nervous System | Jan E. Leestma, MD, MM and Joel B. Kirkpatrick, MD | 619 |
| 9 | Forensic Aspects of Complex Neural Functions | Jan E. Leestma, MD, MM | 659 |
| Index | 709 | ||
Excerpts from the book:
This book has become a classic over the years. Here are some excerpts from the book, so reader can get some ideas as to what is contained within the book. Here is what Leestma has to say about Intracranial Hypertensive Hemorrhage (pages 97 - 104)...
 |
This form of cerebral hemorrhage of usually massive proportions accounts for at least 52% of fatal cases of subarachnoid hemorrhage (SAH) but has been decreasing over the past 20 years; in fact, the rate of decrease has now flattened out [52, 101-103]. The fatality rate is high (90% of victims die within 72 hours of onset of symptoms), and only a small percentage survive even in the face of surgical treatments. Persons affected are generally older than 40 years (more than 75%), with about 25% of cases occurring in each succeeding decade. Males and females are about equally affected. Cerebral hemorrhages that occur in young people appear to have a slightly different demographic than in older victims [104]. Typical symptoms of acute intracerebral hemorrhage are usually stroke-like, sudden, and occur at all times of the day and in association with all forms of activity, in much the same pattern as rupture of berry aneurysms. There may be an associated sudden headache, an urge to vomit or use the toilet (many victims are found in the bathroom), a rapidly progressing hemiparesis, and rapid loss of consciousness. Death rarely occurs within 1 hour and can be protracted if the victim is transported to the hospital and ventilatory support provided.
Surgical treatment of hypertensive hemorrhages, with the exception of those with cerebellar hemorrhages [105, 105a] who have stabilized, is generally not rewarding. In some cases of basis pontis hemorrhage, protracted coma in the locked-out state may occur [13, 106] with little chance that a surgical intervention is useful. The common locations for such hypertensive hemorrhages are first and foremost (about 80% of cases) within the basal ganglia (usually in the lateral ganglionic region involving the globus pallidus and external capsule region), followed in about equal amounts (about 10% each) by hemorrhages in the basis pontis [107] and in the cerebellar hemispheres involving the dentate nucleus.
 |
Multiple hemorrhages or hemorrhages in other locations will probably have an etiology other than hypertension, which should be investigated.
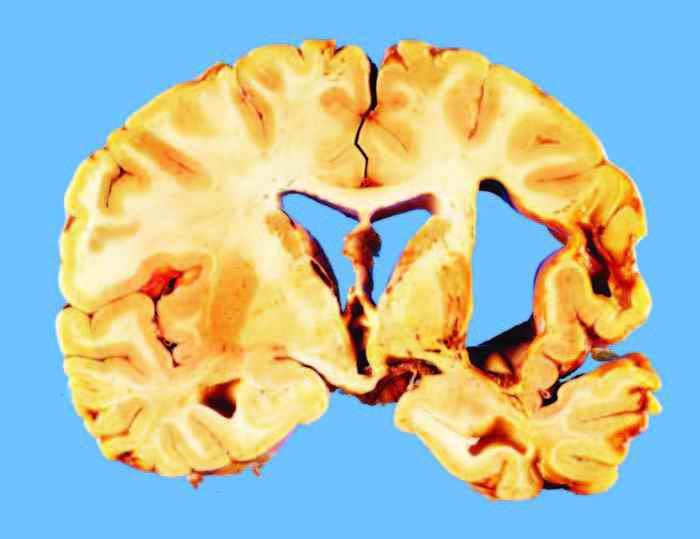
In so-called lateral ganglionic hemorrhage, as illustrated in Figures 3.7 and 3.8, the site of origin of the hemorrhage appears to be within either the external globus pallidus, the putamen, or the external capsule-claustrum, deep to the insula. The hemorrhage then appears to push the remaining basal ganglia toward the midline and then to dissect upward along the path of least resistance, through the white matter over the caudate nucleus, into the lateral ventricle, or to dissect forward or backward until another ventricular chamber is reached. Occasionally, the primary hemorrhage may occur within the internal capsule or thalamus and rupture directly into the lateral ventricle or third ventricle. On rare occasions, the hemorrhage may be circumscribed and fail to dissect into the ventricle. In this circumstance, the individual may survive and, when coming to autopsy for another or related cause even years later, will show a smooth-walled, brownish or yellow cystic space at the site of the old hemorrhage, as illustrated in Figure 3.9.
Histological examination of the hematoma itself generally is unrewarding; however, adjacent to the hemorrhage or in the opposite basal ganglia, one can usually find the stigmata of hypertensive microvascular disease in the form of sclerotic, tortuous small arterioles within a space that contains a few macrophages or siderophages. Sometimes mineralization or profound collagenization of the perivascular space is seen. Old or recent perivascular hemorrhage (bleeding globes) apart from the main hematoma may also be visible, and occasionally what appear to be true saccular microaneurysms (as described by Charcot and Bouchard in 1868) [108] may be found. It is usually obvious that chronic microvascular disease, not radically different from the typical hypertensive arteriolar sclerosis in the kidneys, is present in several locations. Lacunar infarcts (etat lacunaire) and similar perivascular microinfarcts in the subcortical white matter (etat crible) are also commonly associated.
 |
Commonly associated with ganglionic hemorrhage is a separate hemorrhage in the upper brain stem that results from herniation, often referred to as a Duret hemorrhage (see Figure 3.8), even though this is probably a misnomer [108a]. This hemorrhage most likely occurs when unilateral rapidly developing mass lesions lead to brain stem herniation [109]. Sometimes bilateral mass lesions can produce Duret hemorrhages, but in these cases the evolution of the mass lesions is probably not uniform or in synchrony. A more complete discussion of this lesion can be found in Chapter 5. The hemorrhage may evolve within 30 minutes of the initial catastrophe. Duret hemorrhages are irreversible and mean that restoration of consciousness regardless of treatment is impossible, because the brain stem reticular formation has usually been destroyed. However, vegetative existence may be maintained for some time if ventilatory assistance is available. Survivals from Duret hemorrhages have been reported [110]. An unusual example of an individual who survived a Duret hemorrhage but remained in a vegetative state (locked out) is illustrated in Figure 3.10. The usual course of events, once Duret hemorrhage has occurred and a respirator is in use, is the development of the respirator brain (discussed in greater detail in Chapter 5).
 |
Hypertensive hemorrhages that involve the deep cerebellar gray matter (dentate nucleus) tend to evolve suddenly and often result in relatively prompt loss of consciousness, owing to proximity to the brain stem reticular formation. Likewise, hemorrhages to the base of the pons cause a rapid loss of consciousness by the same mechanism. Cerebellar hemorrhages produce a mass effect that not only produce tonsillar herniations but may also produce upward herniation of the rostral cerebellar vermis through the tentorial notch, as illustrated in Figure 3.11. Cerebellar hemorrhages may rupture into the fourth ventricle and sometimes into the subarachnoid space. These hemorrhages have a high mortality rate, but prompt neurosurgical intervention with evacuation of the clot may be life saving, though neurological deficits may persist.
Primary hemorrhages of the pons involve the basis pontis, as illustrated in Figure 3.12. Such hemorrhages are almost always fatal, but when survivals are prolonged, the individual is usually comatose but may show so-called alpha coma, wherein waking-sleeping EEG patterns may be observed although the victim is deeply comatose [106]. In unusual cases where the hemorrhage is in the distal basis pontis and mass effect or hemorrhage has not damaged the reticular formation, victims of pontine hemorrhages may be conscious but unable to move the extremities or to speak-the so-called locked-in state [13].
 |
 |
Occasionally, it is important in the forensic environment to differentiate between hypertensive hemorrhages and intracerebral hemorrhage due to trauma or some other condition. A practical guide in this situation is that nonhypertensive intracerebral hematomas do not usually occur in the locations where hypertensive hemorrhages are seen (lateral ganglionic region, basis pontis, dentate nucleus of cerebellum). Furthermore, such traumatic hematomas usually underlie the cortical ribbon and are generally smaller than hypertensive bleeds, but they may also be multiple. In apparently traumatic hemorrhages, there may be associated cortical contusions and other evidence of inner brain trauma, such as streak or punctate hemorrhages about the cerebral aqueduct or in the white matter, which should be distinctive. For further discussion of these points regarding physical injury etiologies, see Chapter 6. Forensic issues may arise in cases with cerebral hemorrhages that occur during pregnancy and delivery (with and without eclampsia), with anticoagulation, and in association with drugs of abuse, notably cocaine and amphetamines [104, 111, 112].
It should be borne in mind that individuals with amyloid vascular disease of the brain, a condition whose commonness in elderly individuals [113-116] with or without Alzheimer's disease has been recognized in recent years, may be more vulnerable to traumatic cerebral hemorrhage than other individuals. In fact, it may well be that many of the cases of post-traumatic intracerebral hemorrhages, especially in elderly individuals, are actually cases of amyloid vessel disease that suffered sufficient trauma to cause the affected vessels to bleed (Figure 3.13).
Amyloid angiopathy has been known for many years and was thought to be uncommon or rare [113, 117]. The condition appears to be caused by the apolipoprotein E (APOE) e-2 allele, which causes deposition of B-amyloid in arteriolar walls in the brain but apparently not in other organs of the body. Grossly, if one is suspecting amyloid angiopathy, affected cortical arterial branches may appear somewhat silvery, but generally gross observations are insufficient to make the diagnosis. Microscopic examination of affected vessels shows a thickening of the media and adventitia with a hyaline material (Figure 3.14) that stains positively with Congo red and thioflavine dyes (with ultraviolet microscopy). Sometimes in the center of a hemorrhage due to amyloid vessel disease, one can find a mass of amyloid material (amyloidoma) and evidence of previous hemorrhage and reactions. Usually, surrounding nonhemorrhagic regions will show affected arterioles as well. Affected individuals may hemorrhage many times and sometimes require surgical evacuation of the hematomas, but there is no cure for the condition.
 |
 |
When massive intracerebral hemorrhage not connected with head trauma has occurred and is multifocal or not located in one of the typical sites (lateral ganglionic region, basis pontis, or cerebellar hemisphere) for hypertensive hemorrhage, one of a multitude of other causes must be suspected. The most common of these are diseases of the blood, which include leukemia, polycythemia, hemophilia, thrombocytopenia, disseminated intravascular coagulation (DIC), and sickle cell disease, and overmedication with anticoagulant medications. Other conditions causing similar hemorrhages include delayed deaths in intoxication; fat, bone marrow, and amniotic fluid embolism; disseminated fungal infections (aspergillosis and the other mycelia infections); metastatic choriocarcinoma; melanoma and other neoplasms; cerebral malaria; amyloid vessel disease; and cryptic telangiectatic and other vascular malformations.
Regardless of the underlying disease, the pattern of bleeding is remarkably similar. Especially in leukemia, where a blastic crisis has occurred, hemorrhages are multiple and often lie in the subcortical location in the cerebrum but may involve deep nuclear structures of the basal ganglia, cerebellar white matter, and occasionally the brain stem. The perivascular character of the hemorrhages can often be appreciated on coronal section, where even though the hematoma may be large, it is actually a confluent hemorrhage made up of many adjacent perivascular hemorrhages represented as discrete ball-like bleeds that blend into one another. The basis for such a form of bleeding is massive multifocal destruction of several vessels. Microscopic examination of the transitional zone between normal brain and hemorrhage may reveal the cause of the vessel pathology, be it leukemic infiltration, metastatic tumor, vascular malformation, sickled red blood cells, or intravascular platelet-fibrin thrombi, as in DIC or related conditions. In the case of hemophiliac hemorrhages, microscopic appearances are not especially helpful except to rule out more obvious etiologies.
Leestma has given some highly interesting cases throughout the book. Here is what he has to say in chapter 8 (Gunshot and Penetrating Wounds of the Nervous System) - page 630-1.
 |
 |
Slaughter pistols and stud guns are sometimes chosen for suicide, particularly in Europe, or may occasionally cause serious or fatal wounds in accidental circumstances. The device for stunning large animals at slaughter ejects a plunger by an explosive charge. Because the plunger is captive but does penetrate the brain, the injuries are those of a very lowvelocity missile. Nevertheless, such an injury is often fatal [42-44]. Stud guns or bolt guns are used for construction applications. For safety precautions, the device must have the muzzle firmly depressed against the target or it will not fire. The charge, often a blank .22 caliber cartridge especially designed for this application, propels a nail or other construction material into the work surface, be it wood, metal, or sometimes concrete. Sometimes the nail projectile will penetrate the board or wall and injure another worker or bystander some distance away, or the tool may be used with suicidal intent [44, 45]. An example of a stud gun suicidal injury is illustrated in Figures 8.4 and 8.5.
Rubber and plastic bullets have been used by military and police personnel during riots and in other circumstances where nonlethal forces are required since they were introduced in 1973 [46]. There are a number of designs for the firearms used to propel rubber or plastic projectiles at relatively low velocity that expand in flight or on impact to increase the contact surface area and prevent penetration of the body. In spite of good intentions, numerous fatalities with the supposedly nonlethal projectiles have resulted in well-known areas of past conflict, such as South Africa, Israel and Palestine, and Northern Ireland. Injuries and their severity are a function of the distance between the shooter and the victim, ballistic features of the gun and its projectile, and the site of impact on the body [47]. Penetration of the thorax or abdomen has occurred and can cause death [48], but most fatalities arise from cranial injuries that can cause skull fractures, subdural and epidural hematomas, and even penetrating injuries [49]. Facial and eye injuries are not uncommon but usually are not fatal. Even the relatively low level of fatal injuries from these weapons have prompted many of the forces using them to seek other means of crowd control [49].
The book gives a host of similar information on virtually all aspects of forensic neuropathology. We are sure our readers would enjoy the book as much as we at the journal office did.
 Request a PDF file of this review by clicking here. (If your screen resolution can not be increased, or if printing this page is giving you problems like overlapping of graphics and/or tables etc, you can take a proper printout from a pdf file. You will need an Acrobat Reader though.)
Request a PDF file of this review by clicking here. (If your screen resolution can not be increased, or if printing this page is giving you problems like overlapping of graphics and/or tables etc, you can take a proper printout from a pdf file. You will need an Acrobat Reader though.)
 N.B. It is essential to read this journal - and especially this review as it contains several tables and high resolution graphics - under a screen resolution of 1600 x 1200 dpi or more. If the resolution is less than this, you may see broken or overlapping tables/graphics, graphics overlying text or other anomalies. It is strongly advised to switch over to this resolution to read this journal - and especially this review. These pages are viewed best in Netscape Navigator 4.7 and above.
N.B. It is essential to read this journal - and especially this review as it contains several tables and high resolution graphics - under a screen resolution of 1600 x 1200 dpi or more. If the resolution is less than this, you may see broken or overlapping tables/graphics, graphics overlying text or other anomalies. It is strongly advised to switch over to this resolution to read this journal - and especially this review. These pages are viewed best in Netscape Navigator 4.7 and above.
-Anil Aggrawal

 [ Major links ]
[ Major links ]
[ Aims and Objectives ] [ FAQ ] [ Editorial Board ] [ Contributing Partners ] [ Sitemap ]
[ Paper/Thesis submission guidelines ] [ Editorials - Cumulative Index ] [ Discussion ] [ Chat room ] [ Be our sponsor! ]
[ Cumulative index of Book Reviews sorted by | Publishers | General Interest Books | Technical Books ] [ Animated Reviews ] [ Featured Reviews ] [ E-books ]
[ Reviews with Quizzes ] [ Links ] [ Submit books/journals/software/multimedia for review ] [ journal CD ] [ History of the Journal ] [ Interviews ] [ Credits ]
[ Cumulative index of | Theses/dissertations | [ Online Courses ] [ Awards ] [ Anil Aggrawal's Internet Journal of Book Reviews - Sister Publication ]
[ Cumulative reviews of Software/Multimedia | Books on CD/Audio tapes ] | Calenders | Models ] [ contact us ]
[ Undergraduate section | Postgraduate section ] [ Forensic gadgets/toys/other tidbits ]
Books for review must be submitted at the following address.
Professor Anil Aggrawal (Editor-in-Chief)
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology
S-299 Greater Kailash-1
New Delhi-110048
India
Click here to contact us.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
 IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
Questions or suggestions ? Please use ICQ 19727771 or email to dr_anil@hotmail.com
Page Professor Anil Aggrawal via ICQ

|