Paper 5: Obliquity vs. Discontinuity of ligature mark in diagnosis of hanging - A comparative study by Shrabana Kumar Naik: Anil Aggrawal's Internet Journal of Forensic Medicine: Vol. 7, No. 1 (January - June 2006)
Received: March 29, 2006
Accepted: June 30, 2006
Ref:
Naik SK. Obliquity vs. Discontinuity of ligature mark in diagnosis of hanging - a comparative study.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2006; Vol. 7, No. 1 (January - June 2006): [about 20 p]. Available from: . Published : June 30, 2006, (Accessed:
Obliquity vs. Discontinuity of ligature mark in diagnosis of hanging - a comparative study
by Shrabana Kumar Naik
Assistant Professor,
Department of Forensic Medicine,
Lady Hardinge Medical College,
New Delhi-110001
India
Phone no - 98912-24143 (M), 23408158/23408157 (O)
Email: naikshrabana@yahoo.co.in
Abstract
Although mechanisms of constricting forces acting around the neck of the deceased are different in both hanging and strangulation, still the ligature marks found around the necks appear almost similar. Associated bodily injuries resulting from resistance or violence may not be present in all cases of ligature strangulation. In those cases, it is only the ligature mark that helps us to differentiate hanging from strangulation.
Factors like level, discontinuity and obliquity of the ligature mark, which differentiate hanging from strangulation, are not present simultaneously in all cases of hanging or strangulation. But the ligature mark of hanging must be differentiated from the ligature mark of strangulation before giving opinion; otherwise a serious mistake can result. This can lead to in the conviction of an innocent while a murderer can go unnoticed in the society.
The author, after observing 258 cases of hanging and 8 cases of ligature strangulation, is of the view that obliquity of the ligature mark is the most reliable criterion for differentiating hanging from ligature strangulation, rather than discontinuity.
In the professional life of autopsy surgeon, case of hanging by a ligature is a common encounter. However, suspicion about the mechanism of constriction may arise on more than one occasion. The characteristic finding i.e., the ligature mark found around the neck in both hanging and strangulation creates an element of doubt in many cases. The difficulty increases manyfold when one has to differentiate ligature mark of homicidal hanging from strangulation, as associated bodily injuries will be found on both occasions though in partial hanging it may not be difficult due to absence of marks of violence and resistance.
The ligature mark is a vital piece of evidence, especially when the killer has taken away the actual ligature1. Taking the most important finding i.e., ligature mark into consideration, there are a few points like 1) level, 2) discontinuity and 3) obliquity of the ligature mark which differentiate hanging from ligature strangulation.
However, it is a fact that not all these differentiating features are present simultaneously in all cases of hangings or strangulations. In practice, the distinction between the two groups is important because strangulation is usually homicidal and hanging in vast majority is considered to be suicidal2. So there is always a necessity to differentiate hanging mark from strangulation mark before giving an opinion otherwise an error in judgment can convict an innocent or a murderer can go scot free in the society. Sirohiwal B et al have reported a case of ligature strangulation of a 35year old male that was fabricated as suicidal hanging by the accused3. SK Sharma has reported a case of homicidal hanging of 30 year old female by partial suspension, which was diagnosed as a case of suicidal hanging at the end of autopsy but circumstances on later days changed the entire face of the case4. These problems represent only tip of iceberg where the autopsy surgeon had faced dilemma either during autopsy or after submission of autopsy report or the law agencies had faced difficulty in solving the cases.
Considering the difficulty in diagnosing ligature mark of hanging and strangulation faced on many occasions, the author has made an attempt to establish the most reliable factor for differentiating ligature mark of hanging from ligature mark of strangulation.
Material & Methods
A total of 266 autopsies wee conducted by the author in death cases due to hanging and ligature strangulation at the Departments of Forensic Medicine of S.C.B.Medical College, Cuttack and Lady Hardinge Medical College, New Delhi within the period of August 1995 to February 2006.
Information regarding the cause of death, manner of death, positions of the dead bodies during police inquest were gathered from the police records and accompanying relatives of the deceased. Irrespective of information collected, both external and internal post-mortem findings were observed meticulously, especially the ligature mark to diagnose hanging or strangulation. Whenever there is any doubt, spot visits were made to ascertain the fact.
During observation of the ligature mark, all the parameters like its level, discontinuity and obliquity were noticed. When ligature was found around the neck during autopsy or sent separately by the police, nature of ligature and type of applied noose were taken into account for complete evaluation.
The findings thus obtained in all these cases were put in a tabular form in relation to all the factors, differentiating hanging from ligature strangulation.
Observation & Analysis
Suicidal
hanging
252
Homicidal hanging
6
Ligature Strangulation
8
Total
266
Table 1: Number and types of cases
As is clear from above, out of 266 death cases, 252 victims had died due to suicidal hanging, 6 victims due to homicidal hanging and rest 8 victims had died as a result of ligature strangulation.
Type
Partial
hanging
Complete
hanging
Total
Suicidal hanging
13
214
227
Homicidal hanging
3
3
6
Total
16
217
233
Table 2: Partial/complete hanging of victims in hanging cases
Out of 233 cases, 16(6.86%) victims had died due to partial hanging where as 217(93.13%) victims had died due to complete hanging.
Mode
Noose with fixed knot
Noose with slipping knot
Loop without knot/ Knot without loop/Absence of loop or knot
Total
Suicidal hanging
11
57
98
166
Homicidal hanging
0
6
0
6
Ligature Strangulation
7
0
1
8
Total
18
63
99
180
Table 3: Types of noose/knot applied
In 180 cases where the ligature materials were available either around the neck or by the police, noose with fixed knot was present only in 11 cases of suicidal hanging. Noose with slipping knot found in 57 cases of suicidal hanging as well as in all homicidal hangings. Loop without knot, knot without loop or absence of both loop and knot were found in 98 cases of suicidal hanging. However, in cases of ligature strangulation, except one all others had noose with fixed knot.
Figure 1. Figure shows the level of ligature mark higher in the neck in case of suicidal hanging.
(Click picture to enlarge)
Site
Suicidal
hanging
Homicidal
hanging
Ligature
Strangulation
Total
Above LP*
157(62.3%)
4(66.66%)
1(12.5%)
162
On LP
52(20.63%)
1(16.66%)
0(0%)
53
On & above LP
31(12.3%)
1(16.66%)
3(37.5%)
35
Below LP
12 (4.76%)
0(0%)
4(50%)
16
Total
252
6
8
266
Table 4: Level of constricting force/ligature mark (*LP = Laryngeal prominence)
Considering the level of constriction represented by ligature mark, it was found to be situated on or above the level of laryngeal prominence in most cases of suicidal hanging (Figure 1) and all cases of homicidal hangings. Ligature mark was found below the level of laryngeal prominence in 12 (4.76%) cases of suicidal hanging most of which were partial hangings.
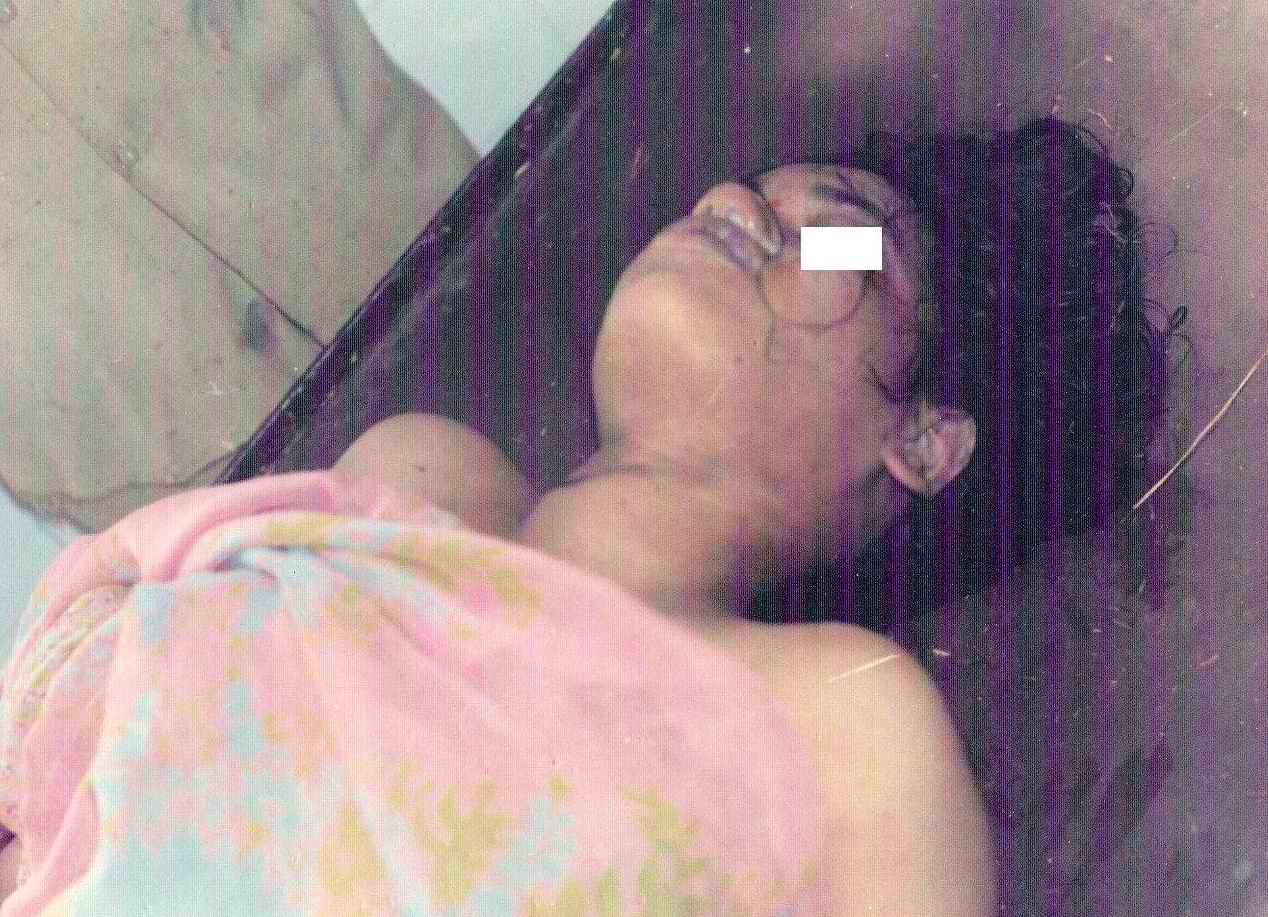
Figure 2. This picture shows the level of ligature mark higher in the neck even in case of ligature strangulation, belying the classical belief that ligature mark in strangulation must be below the thyroid cartilage.
(Click picture to enlarge)
On the other hand, in strangulation, ligature mark was observed below the level of laryngeal prominence in 4(50%) cases. The rest 50% cases showed mark on or above the level of laryngeal prominence (figure 2).
Discontinuity
Suicidal
hanging
Homicidal
hanging
Ligature
Strangulation
Present
224 (88.89%)
4 (66.66%)
0 (0%)
Absent
28 (11.11%)
2 (33.33%)
8 (100%)
Total
252
6
8
Table 5: Discontinuity along the course of ligature mark
Figure 3. This picture shows discontinuity on the right lateral aspect of neck at the site of knot in case of suicidal hanging. (Click picture to enlarge)
Figure 4. This picture shows discontinuity on the left anterolateral aspect of neck at the site of knot in case of suicidal hanging. (Click picture to enlarge)
Figure 5. This picture shows discontinuity of ligature mark on the anterolateral aspects of neck (on both sides) in case of homicidal hanging. (Click picture to enlarge)
Considering discontinuity along the course of ligature mark, it was found as a common feature in most of the suicidal as well as homicidal hangings (Figures 3, 4 and 5). However, discontinuity in the mark could not be detected in 28 (11.11%) cases of suicidal hanging and 2 (33.33%) cases of homicidal hanging.
Figure 6. This picture shows continuous and overriding ligature mark at the back of neck in a case of ligature strangulation. (Click picture to enlarge)
Absence of discontinuity along the course of ligature mark was noticed in all cases of ligature strangulation (Figure 6).
Direction
Suicidal
hanging
Homicidal
hanging
Ligature
Strangulation
Oblique
252 (100%)
6 (100%)
0 (0%)
Horizontal
0 (0%)
0 (0%)
8 (100%)
Total
252
6
8
Table 6: Direction of course of the ligature mark
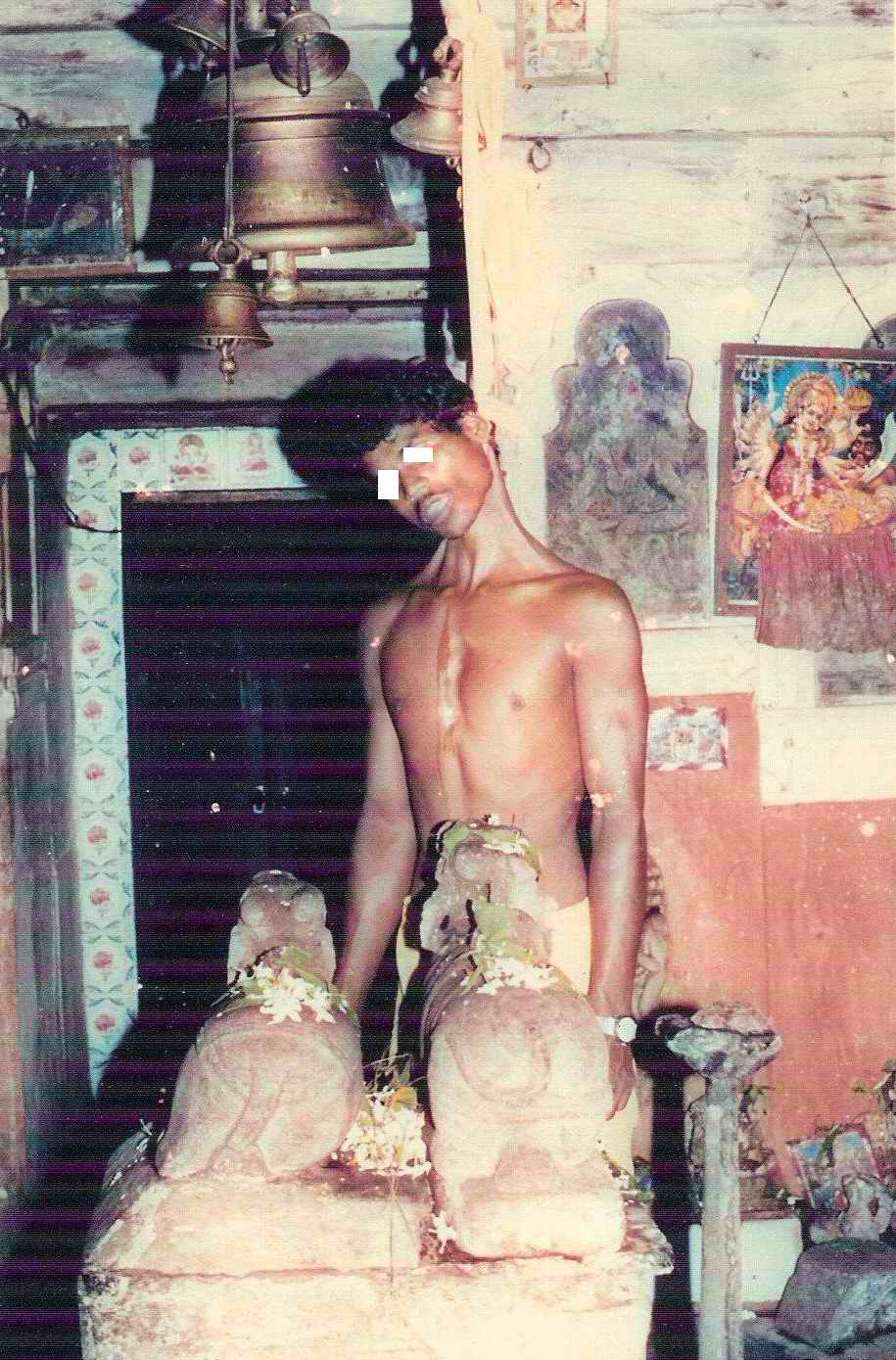
Figure 7. Figure showing oblique ligature mark in case of suicidal hanging. (Click picture to enlarge)
Figure 8. This picture shows obliquely placed ligature even in case of partial hanging. (Click picture to enlarge)
Figure 8a. This figure shows obliquely placed ligature in the same case as above. (Click picture to enlarge)
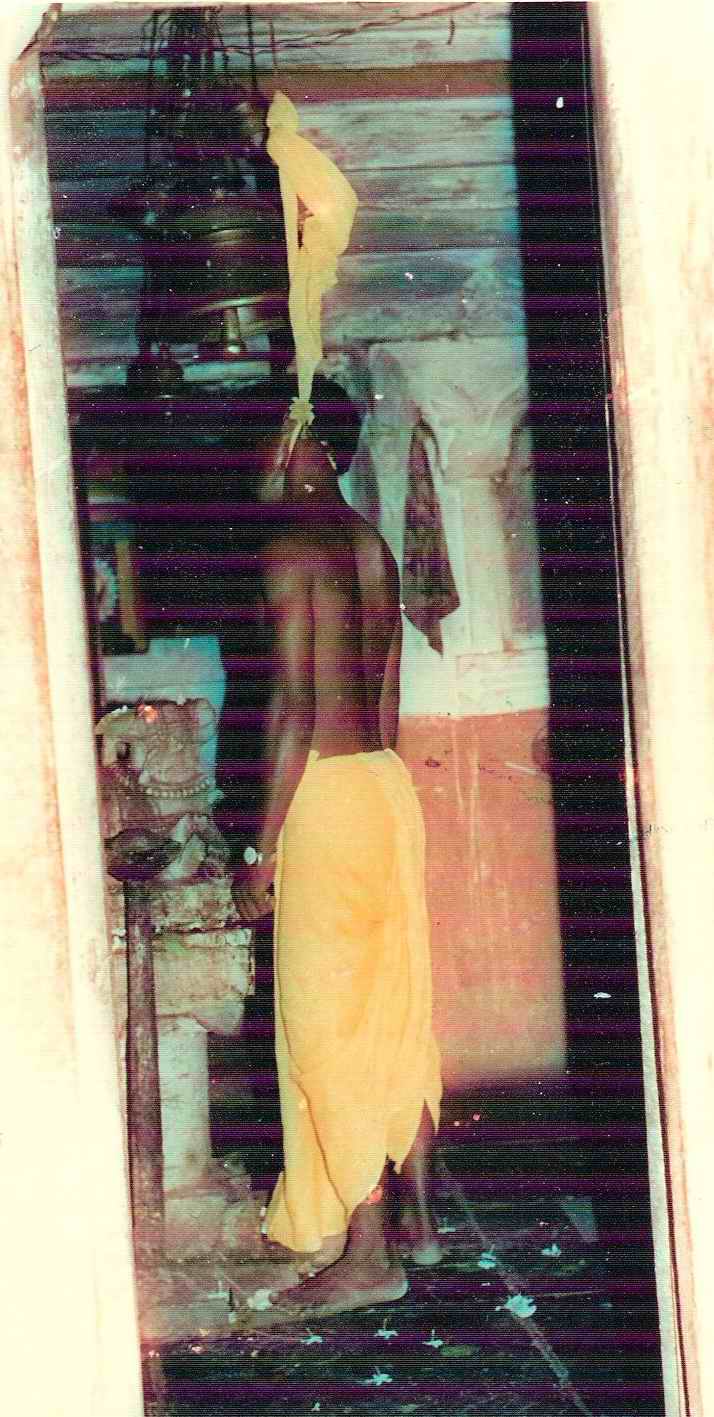
Figure 9. This pictures shows a case of partial hanging in sleeping position. Obliquity of ligature mark was detected even in such degree of partial suspension. (Click picture to enlarge)
When the direction of course of the ligature mark was considered, it was found to be oblique at least near the site of knot in all cases of suicidal hangings (Phographs-7, 8, 8a and 9) as well as homicidal hangings.
Figure 10. This picture shows a case of ligature strangulation where ligature mark appears to be oblique, due to use of very hard ligature like metallic wire. Otherwise it was horizontal around the neck. (Click picture to enlarge)
On the contrary, horizontal ligature mark was noticed in all cases of ligature strangulation (Figure 10).
Discussion
Differentiating between hanging and strangulation is an age old problem3. While diagnosing a case of death resulting from constriction of neck by applying a ligature, three important parameters i.e., level, discontinuity and obliquity of ligature mark are always considered to differentiate hanging from strangulation.
It is a well-accepted fact that the ligature mark of hanging and strangulation are not found at same level. Authors have reported that hanging mark is situated higher in the neck usually above the laryngeal prominence.1,5,7,8,9
Where suspension point is low, the resulting mark may be set at a lower level typically immediately above or below the laryngeal prominence.
5,6,78
Jason PJ et al have reported that position of mark of hanging depends on how the device was fixed and the suspension point.6 Reddy KSN has mentioned that mark of hanging is situated above the level of thyroid cartilage, between larynx and chin in 80% cases. It may be situated at the level of thyroid cartilage in about 15% cases and below the level of thyroid cartilage in about 5% cases, especially in partial suspension.9 In the present study, it was observed that ligature mark was on or above the level of laryngeal prominence in most cases of suicidal and homicidal hanging. However, it was found below the level of laryngeal prominence in 4.76% cases of suicidal hanging most of which were partial hangings. In cases of ligature strangulation, mark was found below the level of laryngeal prominence only in 50% cases whereas in rest 50% it was on or above the level of laryngeal prominence.
What is already known on this topic
Generally, death from hanging is presumed to be suicidal whereas death from ligature strangulation is presumed to be homicidal. Ligature mark found around the neck is the most characteristic finding noticed in both manners of death. As the ligature marks found in both forms of asphyxial deaths appear similar; factors like obliquity, discontinuity and level of ligature mark round the neck are taken into consideration, to differentiate hanging from ligature strangulation. However, typical descriptions made about ligature marks of hanging and ligature strangulation in most of the available forensic medicine textbooks are not seen in all cases of hanging or strangulation, thus posing problem for diagnosing the case of hanging or strangulation. The problem aggravates in cases of partial hanging (ligature mark is seen almost horizontally and at lower level), use of well slipping noose or very tightly fixed noose in hanging (ligature mark is found continuous) and pulling ligature backwardly and upwardly in ligature strangulation (obliquely placed ligature mark).
What this paper adds
A clear diagnosis about the ligature mark of hanging and ligature strangulation must be reached before giving opinion, to avoid miscarriage of justice. Present study shows that obliquity along the course of ligature mark round the neck is most important criteria to differentiate hanging from ligature strangulation than other factors like level and discontinuity. Presence of marks of violence and resistance on the dead body only indicate homicidal nature of the death, not the manner of constriction of neck.
It is also well known fact that discontinuity along the course of the ligature mark is another important criterion while describing ligature mark of hanging or strangulation. Authors have mentioned that hanging mark almost never completely encircles the neck.1,5,6,7,8,9
However, when a slipping knot is used, then it may cause the noose to tighten and squeeze the skin through the full circumference of the neck.
1,5,6,7,8,9
In most instances, the point of suspension is indicated by a gap in the skin mark. In strangulation, unless the killer is pulling upwards, there will be no gap in the mark. However, there can be discontinuity along the course of ligature mark due to interposing clothing, scalp or beard hairs or fingers of the victim in both hanging and strangulation.5 In the present study, it was noticed that though discontinuity of the mark was a common feature in most cases of suicidal as well as homicidal hanging still it was missing in 11.11% cases of suicidal hanging. In strangulation deaths, discontinuity of the ligature mark was not present even in a single case.
Observation is incomplete when obliquity along the course of the ligature mark is not noted in cases of hanging and strangulation. Authors have reported that hanging mark is situated obliquely across the circumference of neck.
5,7,8,9
Where suspension point is low, the pull on the rope is almost at right angle to the axis of the body, so the resulting mark may be almost horizontal. In strangulation, unlike hanging, the mark tends to encircle victim's neck horizontally. However, the mark may be oblique as in hanging, if the victim has been compressed by a cord while in recumbent posture, or if the victim was sitting and the assailant applied the ligature on the neck while standing behind victim, thus using the force backward and upward.
7,9
Simpson K has opined that the mark of hanging usually rises to a 'peak' pointing the junction of the noose and vertical part of the ligature, this being a distinguish feature from ligature strangulation. However, exceptions occur if the suspension point is low, a horizontal mark may be produced which can be confused with strangulation. In strangulation, the mark is usually horizontal and will not show any rising peak to a suspension, as do many hangings. Present study revealed that obliquity along the course of ligature mark was a constant feature in all deaths due to hanging irrespective of their manner of suspension whether homicidal or suicidal. In ligature strangulation, horizontal ligature mark was observed in all cases.
None of us will disagree that the number of deaths due to ligature strangulation are rare in comparison to hanging. Therefore, the variations to the characteristics of ligature mark of strangulation are rather very rare to meet. Taking the variations seen in the ligature marks of hanging, the present study establishes that some sort of obliquity is always present in the ligature mark of hanging which can be detected at least near the site of knot in the form of continuous or non-continuous inverted '' V ''. It is evident even in partial hanging as the factor of suspension differentiates hanging from strangulation.1
Conclusion
This study categorically shows that obliquity in the course of ligature mark being directed upwards to the knot position is a better criterion for diagnosis of hanging than the factor of discontinuity which may not be present in all cases of hanging. The author feel necessary to stress that presence of other bodily injuries due to resistance and/or violence besides the ligature mark around the neck suggests only homicidal death not about the manner of constriction.
It can be thus concluded that the presence of discontinuity along the course of ligature mark is highly suggestive of hanging but its absence neither rules out hanging nor concludes strangulation. Therefore, based upon the low level of ligature mark and absence of discontinuity, opinion as a case of ligature strangulation should not be given in haste unless obliquity along the course of ligature mark is completely ruled out. Whenever doubt persists, it should be in favour of hanging.
(2) Taylor AS. (1984) Taylor 's principles and Practice of Medical Jurisprudence, 13th ed. by Mant AK., B.I. Churchill Livingstone, p.303-319. (Back to [citation] in text)
(3) Sirohiwal B.L., Paliwal P.K., Bharat Bhushan, Yadav D.R (2001). A Case Of Strangulation Fabricated As Hanging. Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology, 2001; Vol. 2, No. 2 (July-Dec 2001): http://www.geradts.com/anil/ij/vol_002_no_002/papers/paper005.html; Published November 29, 2001, (Accessed: February 24, 2006) (Back to [citation 1]
[citation 2] in text)
(4) Sharma, SK (2000). Homicidal Hanging - Case Report (Bias In Premise Of Hanging). Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology, 2000; Vol. 1, No. 1 (Jan-Jun 2000): http://www.geradts.com/anil/ij/vol_001_no_001/paper001.html; Published: February 21, 2000, (Accessed: February 24, 2006) []
(Back to [citation] in text)
(6) Jason PJ, Anthony B, William S.(2003) Forensic Medicine-Clinical and Pathological Aspects, Greenwich Medical Media Ltd, London, 1st ed. P.266-269 (Back to [citation 1]
[citation 2]
[citation 3]
[citation 4]
in text)
N.B. It is essential to read this journal - and especially this paper as it contains several tables and high resolution graphics - under a screen resolution of 1600 x 1200 dpi or more, and preferably on a 17" or bigger monitor. If the resolution is less than this, you may see broken or overlapping tables/graphics, graphics overlying text or other anomalies. It is strongly advised to switch over to this resolution to read this journal - and especially this paper. These pages are viewed best in Netscape Navigator 4.7 and above.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
 Naik SK. Obliquity vs. Discontinuity of ligature mark in diagnosis of hanging - a comparative study.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2006; Vol. 7, No. 1 (January - June 2006): [about 20 p]. Available from:
. Published : June 30, 2006, (Accessed:
Naik SK. Obliquity vs. Discontinuity of ligature mark in diagnosis of hanging - a comparative study.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2006; Vol. 7, No. 1 (January - June 2006): [about 20 p]. Available from:
. Published : June 30, 2006, (Accessed:
 Email Dr. Naik by
Email Dr. Naik by 








 This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
 IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER

