Paper 3: Kronlein Shot - A Rare Presentation Of A Firearm Injury Of The Head. by Basant Lal Sirohiwal, Daya Sirohiwal, Luv K. Sharma, P. K. Paliwal, Swati Sirohiwal: Anil Aggrawal's Internet Journal of Forensic Medicine: Vol. 9, No. 1 (January - June 2008)
Received: April 18, 2007
Accepted: December 14, 2007
Ref:
Sirohiwal, BL, Sirohiwal, D, Sharma, LK;
Paliwal, PK, Sirohiwal, S. Kronlein Shot - A Rare Presentation of A Firearm Injury of The Head.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2008; Vol. 9, No. 1 (January - June 2008): [about 7 p]. Available from: . Published : January 7, 2008, (Accessed:
Email the corresponding author Basant Lal by clicking here
Basant Lal
(Click to enlarge)
Kronlein Shot - A Rare Presentation of a Firearm Injury of the Head
by Basant Lal Sirohiwal,* Daya Sirohiwal,** Luv K. Sharma,*** P. K. Paliwal,@ Swati Sirohiwal,@@
*Professor, Forensic Medicine, Pt. B.D. Sharma PGIMS, Rohtak, India.
**Professor, Gynaecology and Obstetrics, Pt. B.D. Sharma PGIMS, Rohtak,India.
***Associate Professor, Forensic Medicine, Pt. B.D. Sharma PGIMS, Rohtak, India,
@Professor & Head, Forensic Medicine, Pt. B.D. Sharma PGIMS, Rohtak, India,
@@III yr MBBS student, All India Institute of Medical Sciences, New Delhi, India,
*Corresponding author Basant Lal Sirohiwal Tel. 09896016532 (mobile), 951262-212873 (Res), e-mail: drbasantsri@gmail.com
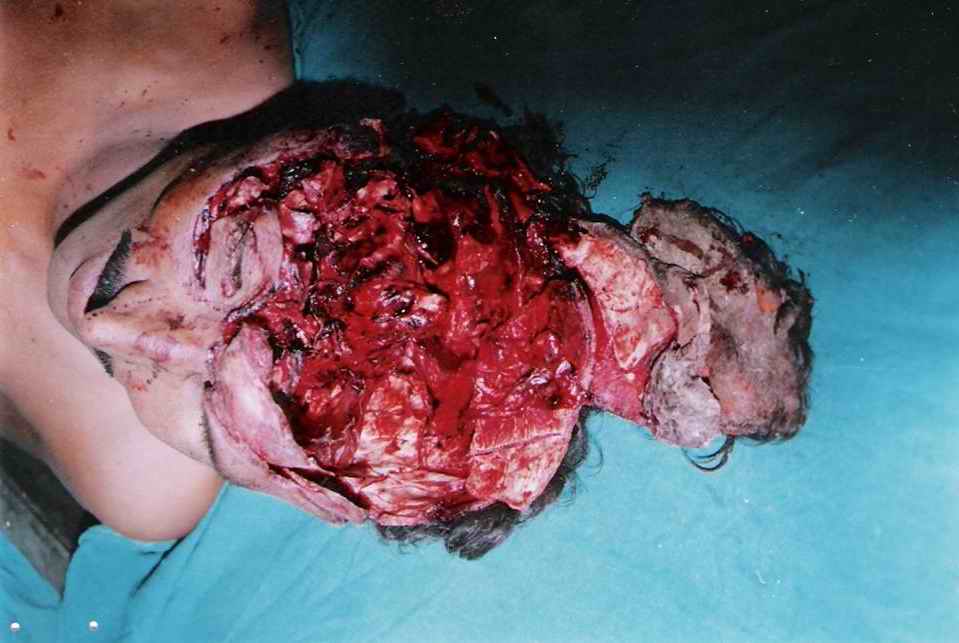
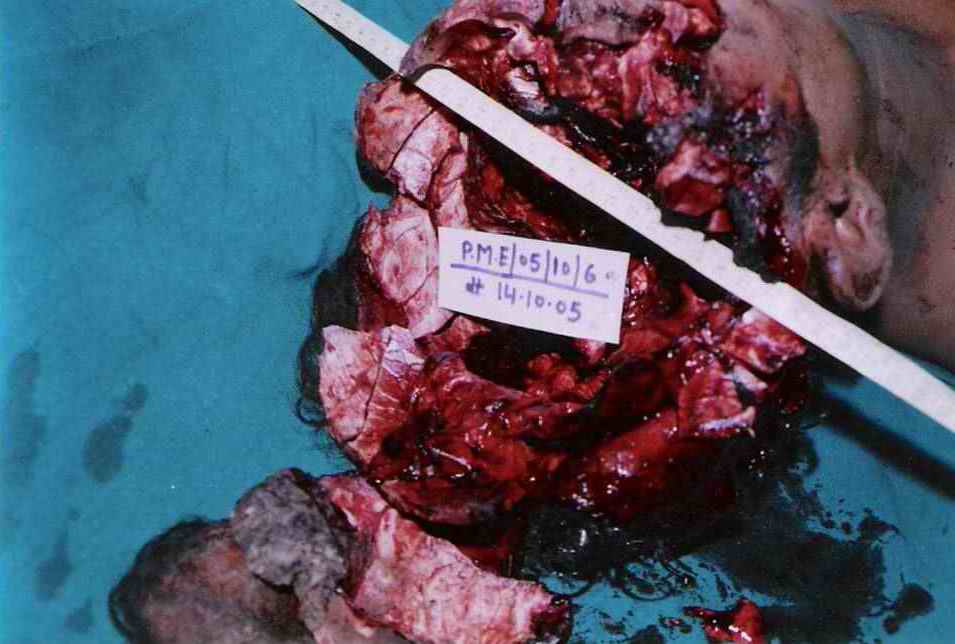
Picture 1a (top) and 1b (bottom): Pictures showing exploded calvarium with multiple fragments of skull bones attached with scalp on the back of the head. Both cerebral hemispheres were missing. [Click all pictures to enlarge]
Abstract
The authors present a rare case of Kronlein shot, which can mimic an explosion injury and can often cause confusion among the law enforcement authorites, as well as among the less experienced forensic pathologists. The author explain how such injuries can be reconstructed.
Firearm injuries may produce several atypical effects, one of the most bizarre of which is the Kronlein shot. To understand the physical mechanics of Kronlein shot, it is important to appreciate that the kinetic energy of a bullet passing through a body is utilized (or consumed) in the following five phenomena (in chronological sequence).
To travel from the cartridge upto the tip of the muzzle and then upto the victim's body.
To overcome and break the resistance of skin, bones and other tissues at the site of entrance.
To push the tissues aside (radial displacement), during the course of the bullet within the body.
To overcome and break the resistance of skin, bones and other tissues at the site of exit.
To travel from the exit of the wound upto the point where the bullet is finally found and recovered by the law enforcement authorities
How the bullet spends its energy in each of the above five parts is determined strictly by the laws of physics. For instance it is a logical impossibility for the bullet to spend energy at, say, level 3 (used to push the tissues aside), without spending at least some energy at lower levels. It is quite possible that the bullet passes through such tough parts (a thick skull for example), that most of its energy is already consumed and hardly any is left to push the tissues aside. If however less energy is consumed in overcoming the tissues at the entrance, relatively more energy would be available in displacing the tissues aside. In the case of skull and brain, this energy (that consumed in producing cavitation) can sometimes be so excessive that it may mimic an explosion, giving rise to the so-called kronlein shot.
Case Report
Picture 2a (top) and 2b (bottom): Pictures depicting the lower arc of a firearm entry hole (punched in) on the left temporal region without effects of powder blast and with extruded calvarium. [Click all pictures to enlarge]
An alleged case of firearm death was referred to the authors. It mimicked injury caused by an explosion, and if the case was that caused by a firearm (as alleged by the police), the main difficulty or the challenge before the authors was to find the entry and exit wounds, which were obliterated due to the explosive effects. On internal examination, both cerebral hemispheres were found to be missing. However cerebellum below tentorium was intact. The injury was reconstructed by approximating the extruded margins of the scalp. Upon reconstruction, both entry and exit wounds could be seen easily. Firearm entry and exit wounds in the skull was having characteristics of punched in and punched out margins respectively. Both entry and exit wounds in the scalp were found to be in line with the corresponding defects in the skull. The case was that of a typical Kronlein shot.
Picture 3: Showing beveled punched out margin of the entry hole (inner table of left temporal bone). [Click all pictures to enlarge]
Discussion
As mentioned above, the energy spent at level 3 (used to push the tissues aside), is mainly utilized in the formation of a cavity (primary cavitation), which - depending on the kinetic energy of the bullet - may be as large as 4-5 times the diameter of the bullet. In the case of brain, this may cause the brain to suddenly bulge in an outward radial direction and strike at the inner aspect of skull with great force. As the bullet passes, this primary cavity collapses, and is followed by a secondary cavitation (partly as a result of oscillation of tissues). This secondary cavity has a negative pressure, which sucks debris from the tissues around into the track.
Events during the state 3 (when the bullet is passing through the brain) need some detailed consideration for a proper understanding of Kronlein shot. During stage 3, the brain is expanding outwards with great force, as already described. If the skull is intact - as is usually the case - the outer surface of the brain may suffer extensive contusions, as it strikes the inside of the skull. In rare cases, if the skull is fractured extensively, the brain does find an exit, and the force may be sufficient to throw it out of the skull (Kronlein shot). In some cases, the brain has been found at quite a distance from the body. In one case, the brain has been described perched on a tree nearby in an almost intact condition!
Kronlein shot is thus produced when a remarkable sequence of events happens. When the energy of the missile is too great (as happens in rifle shots fired from close range), enough energies are available for steps 2, 3 and 4. Enough energies consumed at step 2 and 4 result in extensive fractures of the skull at entry and exit. If the fractures are extensive, they may even unite together, opening the skull completely and setting a perfect stage for the brain to be thrown out. Enough energy spent at step 3 results in the formation of a very severe cavitation, and the brain expanding outwards with great force. This combination of brain expanding outwards with great force and a completely opened skull (due to union of entry and exit wounds of the skull), causes the brain to be thrown outside with great force. This is the typical Kronlein shot.
Conclusion
Forensic pathologists may sometimes be presented with a firearm injury case, which may mimic explosion. It is very easy to be misled and think that the police is lying. However on careful reconstruction of the wound and a visit to the scene of crime (where bullet and cartridge may be recovered), the true nature of the cause of death may be inferred. Thus the importance of reconstruction of wound and visit to the scene of crime is vital in all cases of suspected Kronlein shot.
N.B. It is essential to read this journal - and especially this paper as it contains several tables and high resolution graphics - under a screen resolution of 1600 x 1200 dpi or more, and preferably on a 17" or bigger monitor. If the resolution is less than this, you may see broken or overlapping tables/graphics, graphics overlying text or other anomalies. It is strongly advised to switch over to this resolution to read this journal - and especially this paper. These pages are viewed best in Netscape Navigator 4.7 and above.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
 Sirohiwal, BL, Sirohiwal, D, Sharma, LK;
Paliwal, PK, Sirohiwal, S. Kronlein Shot - A Rare Presentation of A Firearm Injury of The Head.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2008; Vol. 9, No. 1 (January - June 2008): [about 7 p]. Available from:
. Published : January 7, 2008, (Accessed:
Sirohiwal, BL, Sirohiwal, D, Sharma, LK;
Paliwal, PK, Sirohiwal, S. Kronlein Shot - A Rare Presentation of A Firearm Injury of The Head.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2008; Vol. 9, No. 1 (January - June 2008): [about 7 p]. Available from:
. Published : January 7, 2008, (Accessed:
 Email the corresponding author Basant Lal by
Email the corresponding author Basant Lal by 



 This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
 IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER


