Paper 2: The Venous Sinus Appears To Be a Source of Pulmonary Thrombosis by Katsuji Nishi and colleagues: Anil Aggrawal's Internet Journal of Forensic Medicine: Vol. 11, No. 2 (July - December 2010)
Received: June 25, 2009
Received in revised form: October 28, 2009
Accepted: October 28, 2009
Ref:
Nishi, K., Sakaguchi, I., Nakagawa, T., Naitoh, S., Takaka, N., Hirano, A., Takase, I., Yamamoto, Y. The Venous Sinus Appears To Be a Source of Pulmonary Thrombosis.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2010; Vol. 11, No. 2 (July - December 2010): [about 6 p]. Available from: . Published : July 1, 2010, (Accessed:
The Venous Sinus Appears To Be a Source of Pulmonary Thrombosis
by Katsuji Nishi, Ikuo Sakaguchi, Tokiko Nakagawa, Shiho Naitoh, Naoki Takaka, Ai Hirano, Izumi Takase, Yoshio Yamamoto
Department of Legal Medicine,
Shiga University of Medical Science,
Shiga,
Japan
Abstract
Figure 1. Tattoos all over the body of the deceased (A). At the time of his death, the deceased was working at a tattoo parlor and presumably had been practicing on his own body, especially in legs (B and C). [Click all pictures to enlarge]
Pulmonary thrombosis is a common complication caused by venous thrombosis in the deep veins in the legs. In contrast, the occurrence of cerebral venous and pulmonary thrombi without evidence of systemic venous thrombosis is unusual. We performed an autopsy on a 32 year-old man found dead in his living room. The autopsy revealed massive pulmonary thrombi and organized thrombus in the right transverse sinus. We confirmed the absence of any thrombus in the veins of the lower limbs, iliac vein and the inferior vena cava. Histological examination showed that the thrombi in the main pulmonary arteries had recently developed and that the thrombus in the sinus and those in the peripheral pulmonary arteries were organized with recanalisation and blood clotting. We concluded that the pulmonary embolism observed in this case was brought on by a cerebral sinus thrombus, and the cause of death was determined as pulmonary thrombosis.
Keywords
Pulmonary Thrombosis, Cerebral Venous Thrombosis.
Introduction
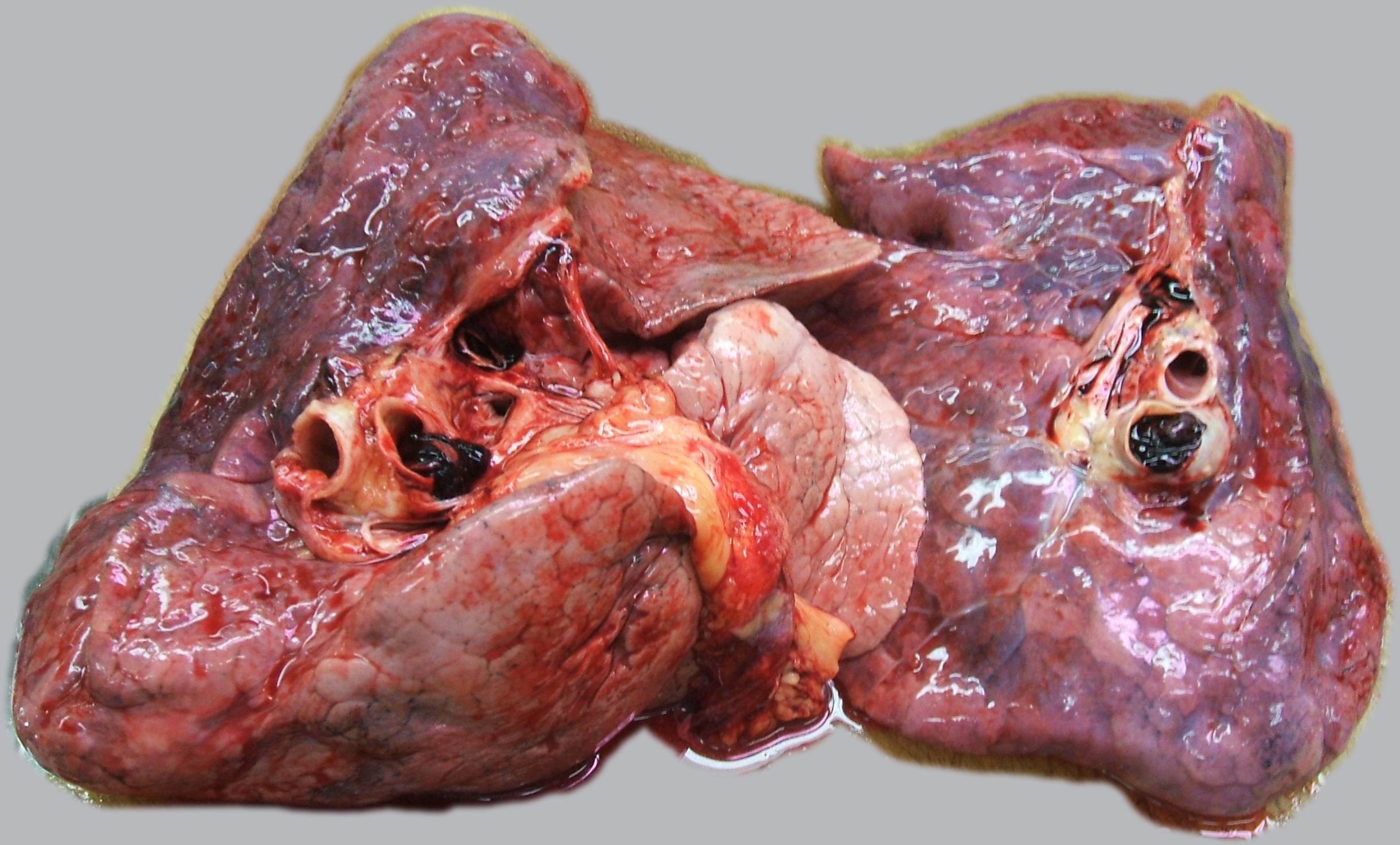
Figure 2. Relatively newly developed thrombi with small amounts of fibrin observed on both pulmonary arteries. [Click all pictures to enlarge]
Cerebral venous thrombosis (CVT) was first recognized in the 19th century1 as an infrequent disease with an often dramatic clinical presentation.2 The epidemiology of the disease has evolved considerable during recent decades with the current predilection involving primarily young and middle-aged people.3 Although the clinical presentation, predisposing factors, neuroimaging findings, and outcomes of CVT are extremely diverse and more than 80 percent of patients have a good neurological recovery,2 the complication of CVT may include coma and/or pulmonary embolism leading to potential sudden death. Diaz et al.4 reported a fatal case of pulmonary emboli from a complication of superior sagittal sinus thrombosis and described that the pulmonary emboli as a complication due to CVT, Thus, this condition appears to have once been well recognized in the literature but has now been largely forgotten. Therefore, we have chosen to report on the autopsy case of a 32 year-old man of which pulmonary emboli was suspected as the fatal complication brought on by a transverse sinus thrombosis.
Figure 3. A brownish-green colored thrombus (arrow heads in A and B) detected in the right-transverse sinus. I am deeply sorry that these pictures are out of focus. After fixing with formalin, the organized thrombus was observed in the transverse sinus (C). [Click all pictures to enlarge]
Case Report
History
One morning, a 32-year-old male was found dead in his living room by his female roommate. He had tattoos all over his body (Fig.1-A) because at that time he was working at a tattoo parlor and presumably had been practicing on his own body (Fig1-B). His roommate stated that he had no prior history of medical illness, although he often complained of headaches since the previous year and of lightheadedness several days before his death. The autopsy was performed the day following his death.
Autopsy findings
The right atrium was enlarged. Removal of the lungs revealed a saddle embolus extending into the lobar branches of both main pulmonary arteries (Fig.2). The thrombus had just recently developed. The liver and kidneys were congested. A relatively hard brown colored thrombus was detected in the right transverse sinus (Fig.3-A and Fig.3-B). No lesions in the brain were observed. We confirmed the absence of any thrombus in the iliac veins and in the inferior vena cava, and in the outer and deep veins of both lower limbs. Unfortunately, we were unable to examine the upper limbs.
Fig.5: This 3D computer graphics is based on histological observation from 40 serial sections. It reveales that the shape of fragment detected in the middle size pulmonary artery of right lung was just like an elephant trunk. This figure is an animation.
[Note: This is a heavy file [17,076 KB]. Please be patient while the animation downloads.]
[This animation will require quicktime player. Get it if you do not have it already]
Histological findings
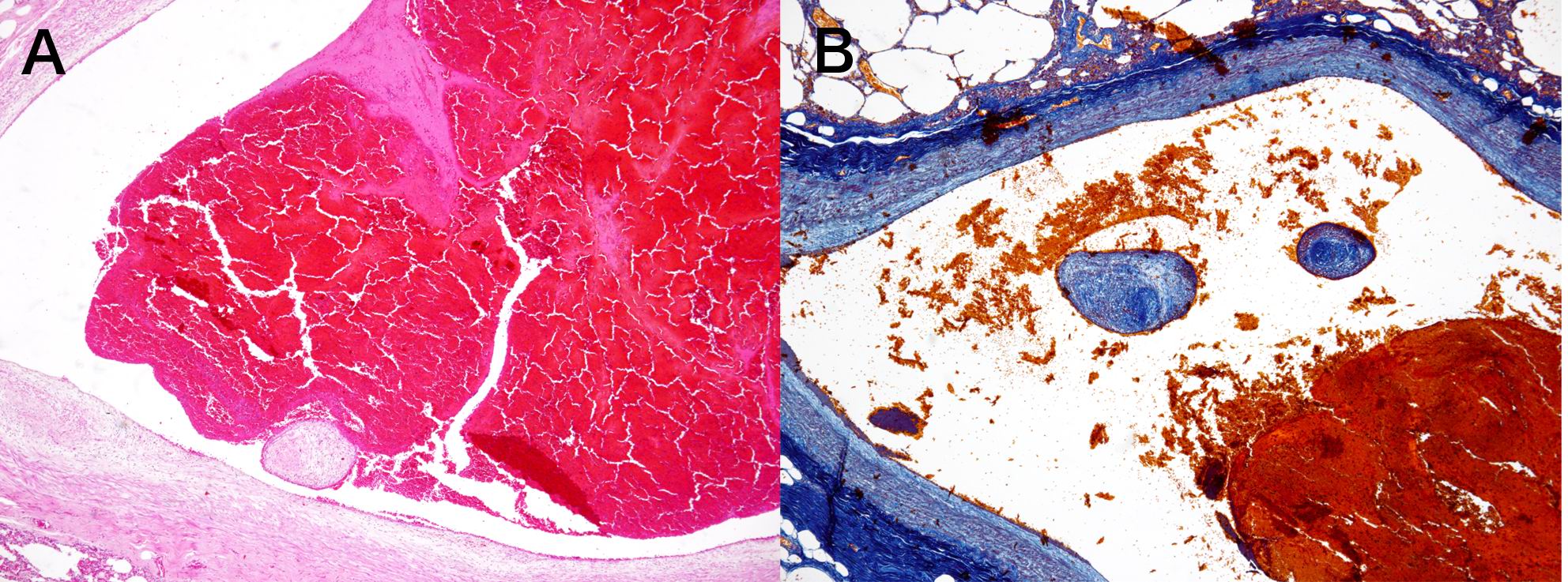
The emboli in the medium-sized pulmonary arteries of the both side lungs mainly consisted of red blood cells and circular fragmented tissues similar to the endothelial tissue, which was recognized around the fresh emboli (Fig. 4-A and Fig. 4-B). The fragmented tissues were faintly adhered to the endothelium in the several sections of a serial 40 sections. The 3D computer graphics based on histological observation from 40 serial sections revealed that the shape of fragment detected in the middle size pulmonary artery of right lung was just like an elephant trunk (Fig.5).
Figure 4. New thrombi detected on the middle size pulmonary arteries of both lungs. The thrombi consisted of an erythrocyte clot and tissue segments, which contained elastic fiber similar to those in endothelial wall of pulmonary artery and hemosiderin pigments similar to those in thrombus in the transverse sinus. The tissue segment slightly adhered to arterial walls only on several sections of the adjacent 40 tissue sections. (A: HE stain, and B: Azan-Mallory stain). [Click all pictures to enlarge]
The thrombus in the right transverse sinus was already organized, and many capillaries in the enlarged vascular epithelial tissue were newly developed. In addition, relatively fresh clots with fibrin and erythrocytes were observed together within the vessel (Fig.6-A, Fig.6-B, Fig.6-C andFig.6- D).
Discussion
Although CVT, deep vein thrombosis, and pulmonary embolism have been associated with thrombophilic defects, CVT is the only condition with the quality of a rare disease. The annual incidence of CVT is 3 to 4 cases per million people. In contrast, deep vein thrombosis and pulmonary embolism affect 1 to 2 people out of 1000 in the general population, annually.5
What is already known on this topic
It is already known that cerebral venous thrombosis is an uncommon cerebrovascular disease presenting with a remarkably wide spectrum of signs and mode of onset. Recent development of diagnostic techniques with imaging machines such as MRI, MRA and CTA increases the ability to detect the cerebral venous thrombosis.
What This study adds
Although there were a few reports concerning fatal cases due to pulmonary thrombosis coming from cerebral sinus thrombosis, in the present case we added the histochemical analysis and 3-D view of the thrombosis in the pulmonary artery.
Suggestions for further development
When the pulmonary thrombosis is observed in autopsies, we should observe deep veins, and cerebral veins and sinuses.
It is still unclear why venous thrombosis mostly occurs in the deep veins of the legs and rarely in cerebral veins or sinus, and why CVT usually occurs at a relatively young age in individuals and more often in women than in men.6 A precise pathogenesis cannot be ascertained in at least 20% to 35% of cases.7 The geographic frequency of CVT was reported as follows: Superior sagittal sinus:62%, Left lateral (transverse) sinus:44,7%, Right lateral sinus:41.2%, Straight sinus:18%, Deep venous system :10%, Cortical veins: 17.1%, Jugular veins:11.9%, Cerebellum veins: 0.3%, Cavernous sinus :13%, respectively, and thrombi were detected in more than one sinus.6
Figure 6. Histological staining revealed that thrombus in the transverse sinus was consisting of organized tissue (A) containing many capillaries (B), a lot of hemosiderin pigments(C) and fibrinous tissue with bleeding (D). Many capillaries showed producing the recanalisation in the organized tissue. [Click all pictures to enlarge]
Concerning the prognosis of CVT, a meta-analysis of ISCVT cohort6 described the prognosis of CVT as more likely than previous reported as the main cause of acute death from transtentorial herniation, secondary to a large hemorrhagic lesion, multiple lesions, or diffuse oedema. Other causes of acute death include status epilepticus, medical complication, and pulmonary embolism.4 Diaz et al.4 reviewed 203 cases of intracranial venous thrombosis between 1942 and 1990 and reported that the mortality rate was 49.3%, and that venous sinus thrombosis was associated with pulmonary emboli in 23 cases and that the mortality rate was 95.6% in those cases.8
In the present case, the thrombus with organized and re-canalized blood vessels in the transverse sinus was remarkably older than those in the pulmonary artery, and the tissue fragment detected in CVT were also observed in the pulmonary artery. Therefore, we believe that the tissue fragments came from the organized emboli in the sinus. Although several cases and retrospective studies have observed the recanalisation phenomena in CVT and the spontaneous occurrence of recanalisation during the first few hours after thrombosis onset in many patients with CVT,9 our subject with recanalisation of CVT showed no significant symptoms except for headache and vertigo until the onset of severe pulmonary embolism.
As thrombi most commonly from in the large, deep veins of the pelvis and lower extremities due to vein circulation, forensic pathologist have to be aware of the other sources of thrombi, specifically in the upper-extremities10 or cerebral sinus when they encounter pulmonary thrombosis.
N.B. It is essential to read this journal - and especially this paper as it contains several tables and high resolution graphics - under a screen resolution of 1600 x 1200 dpi or more, and preferably on a 17" or bigger monitor. If the resolution is less than this, you may see broken or overlapping tables/graphics, graphics overlying text or other anomalies. It is strongly advised to switch over to this resolution to read this journal - and especially this paper. These pages are viewed best in Netscape Navigator 4.7 and above.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
 Nishi, K., Sakaguchi, I., Nakagawa, T., Naitoh, S., Takaka, N., Hirano, A., Takase, I., Yamamoto, Y. The Venous Sinus Appears To Be a Source of Pulmonary Thrombosis.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2010; Vol. 11, No. 2 (July - December 2010): [about 6 p]. Available from:
. Published : July 1, 2010, (Accessed:
Nishi, K., Sakaguchi, I., Nakagawa, T., Naitoh, S., Takaka, N., Hirano, A., Takase, I., Yamamoto, Y. The Venous Sinus Appears To Be a Source of Pulmonary Thrombosis.
Anil Aggrawal's Internet Journal of Forensic Medicine and Toxicology [serial online], 2010; Vol. 11, No. 2 (July - December 2010): [about 6 p]. Available from:
. Published : July 1, 2010, (Accessed:
 Email Dr. Katsuji Nishi by
Email Dr. Katsuji Nishi by 
![Figure 1. Tattoos all over the body of the deceased (A). At the time of his death, the deceased was working at a tattoo parlor and presumably had been practicing on his own body, especially in legs (B and C). [Click all pictures to enlarge]](paper002/hr/1.jpg)
![Figure 3. A brownish-green colored thrombus (arrow heads in A and B) detected in the right-transverse sinus. I am deeply sorry that these pictures are out of focus. After fixing with formalin, the organized thrombus was observed in the transverse sinus (C). [Click all pictures to enlarge]](paper002/hr/3.jpg)

![Figure 6. Histological staining revealed that thrombus in the transverse sinus was consisting of organized tissue (A) containing many capillaries (B), a lot of hemosiderin pigments(C) and fibrinous tissue with bleeding (D). Many capillaries showed producing the recanalisation in the organized tissue. [Click all pictures to enlarge]](paper002/hr/6.jpg)

 This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
This page has been constructed and maintained by Dr. Anil Aggrawal, Professor of Forensic Medicine, at the Maulana Azad Medical College, New Delhi-110002. You may want to give me the feedback to make this pages better. Please be kind enough to write your comments in the guestbook maintained above. These comments would help me make these pages better.
 IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER
IMPORTANT NOTE: ALL PAPERS APPEARING IN THIS ONLINE JOURNAL ARE COPYRIGHTED BY "ANIL AGGRAWAL'S INTERNET JOURNAL OF FORENSIC MEDICINE AND TOXICOLOGY" AND MAY NOT BE REPOSTED, REPRINTED OR OTHERWISE USED IN ANY MANNER WITHOUT THE WRITTEN PERMISSION OF THE WEBMASTER


